Sleep is a critical component of overall health, and insomnia is associated with significant impairment of functioning and quality of life.1 Insomnia is a prevalent condition; in Canada, about 40% experience insomnia symptoms and 13% meet the criteria for chronic insomnia.2 There is also evidence showing that stress and social/environmental disruptions related to the 2020 COVID-19 pandemic have further impacted sleep.3 Even in non-pandemic times, few people with insomnia seek medical consultation for their condition2 —this is almost certainly even more true during the pandemic.
While the definitions and classification of chronic insomnia have shifted somewhat in recent years, the negative sequelae of the disorder highlight the broad-reaching impact of this disorder. That being said, chronic insomnia is treatable. Cognitive behavioural therapy for insomnia (CBTi) is an effective therapy, though prescribed medications are the most widely used options in Canada.2
Chronic insomnia disorder is “characterized by difficulty initiating or maintaining sleep despite adequate opportunity for sleep, with associated distress or impairment of daytime functioning lasting three months or longer for at least three nights each week.”1,4,5 This is in contrast to acute insomnia, which is characterized by sudden onset and duration of less than three months.4
It is important to understand that the current view of insomnia does not distinguish between chronic insomnia as a symptom of another disorder (e.g., depression, anxiety) or as the primary underlying condition. This reflects the reality that in clinical practice, the distinction may be difficult to make, as there is substantial overlap of common symptoms (e.g., sleep disturbance, fatigue, mood, and cognitive problems) between insomnia and mood and anxiety disorders. The current nomenclature of “insomnia disorder” is therefore used for the criteria above. The terms ‘primary’ or ‘secondary’ are no longer in favor; when chronic insomnia co-exists with another condition, the favored term is ‘comorbid insomnia disorder’.6,7
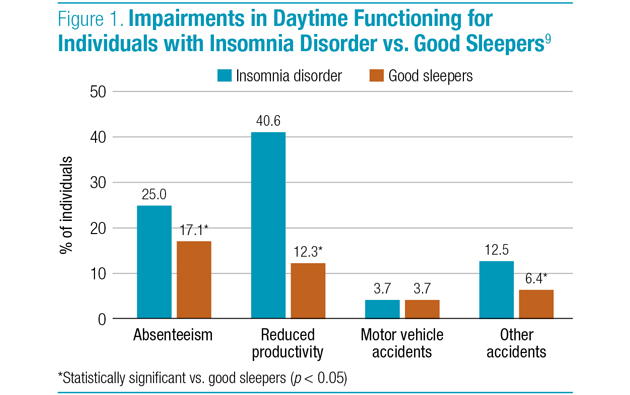
Regardless of the label given to the disorder, it is critical to understand that chronic insomnia can have a broad detrimental impact to individuals and to society as a whole. At the individual level, chronic insomnia can be associated with a wide range of symptoms, such as fatigue, malaise; impairment in attention, concentration or memory; impaired social, family, occupational or academic performance; mood disturbance, irritability, sleepiness, reduced motivation, proneness for errors and overall decrease in quality of life (QoL).1,4-6,8 With respect to functions of daily life, studies have shown that people with insomnia disorder are significantly more likely to report work absenteeism and reduced productivity compared to good sleepers, as well as being more likely to be involved in accidents (Figure 1).9-11
Chronic insomnia is also associated with increased risks of depression and chronic use of hypnotics and, amongst older adults with cognitive impairments, it may hasten placement in nursing home facilities.12-14 With this in mind, identification and appropriate treatment should remain a focus for clinicians.
KEY TAKEAWAYS
Insomnia is not a benign condition, and clinicians should take such complaints seriously in their patient’s evaluation.
Insomnia is a highly prevalent and often a persistent condition, so clinicians should initiate treatment promptly upon careful diagnosis.
Effective treatment options are available, and clinicians should weigh the best option for any given patient as a function of several considerations (e.g., insomnia chronicity, comorbidities).
References:
1. Sateia MJ, Buysse DJ, Krystal AD, et al. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017; 13(2):307–49.
2. Morin CM, LeBlanc M, Bélanger L, et al. Prevalence of Insomnia and Its Treatment in Canada. Can J Psychiatry 2011; 56(9):540-8.
3. Crew EC, Baron KG, Grandner MA, et al. The Society of Behavioral Sleep Medicine (SBSM) COVID-19 Task Force: Objectives and Summary Recommendations for Managing Sleep During a Pandemic. Behav Sleep Med 2020; 1-3.
4. Alberta Guidelines. 2015, Towards Optimized Practice, Assessment to Management of Adult Insomnia - Clinical Practice Guidelines. December 2015.
5. Krystal AD, Prather AA, Ashbrook LH, et al. The assessment and management of insomnia: an update. World Psychiatry. 2019; 18:337–52.
6. Morin CM. Chronic Insomnia: Recent Advances and Innovations in Treatment Developments and Dissemination. Canadian Psychology. 2010; 51(31–9).
7. American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA.
8. Léger D, Morin CM, Uchiyama M, et al. Chronic Insomnia, Quality-Of-Life, and Utility Scores: Comparison With Good Sleepers in a Cross-Sectional International Survey. Sleep Med. 2012; 13(1):43-51.
9. Daley M, Morin CM, LeBlanc M, et al. Insomnia and its relationship to health-care utilization, work absenteeism, productivity and accidents. Sleep Medicine. 2009; 10:427–38.
10. Morin CM, LeBlanc M, Daley M, et al. Epidemiology of insomnia: Prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Med. 2006; 7:123–30.
11. Simon GE, VonKorff M. Prevalence, burden, and treatment of insomnia in primary care. Am J Psychiatry. 1997; 154:1417–23.
12. Breslau N, Roth T, Rosenthal L, et al. Sleep disturbance and psychiatric disorders: A longitudinal epidemiological study of young adults. Biological Psychiatry 1996; 39:411–8.
13. Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA. 1989; 262:1479–84.
14. Katic B, Heywood J, Turek F, et al. New Approach for Analyzing Self-Reporting of Insomnia Symptoms Reveals a High Rate of Comorbid Insomnia Across a Wide Spectrum of Chronic Diseases. Sleep Med. 2015; 16(11):1332–41.
Development of this article was made possible through the financial support of EISAI Ltd. The opinions expressed herein are those of the author and do not necessarily reflect the views and opinions of EISAI Ltd. The author had complete editorial independence in the development of this article and is responsible for its accuracy. The sponsor exerted no influence in the selection of content or material published.