Vivien Brown, MDCM, CCFP, FCFP, NCMP
Assistant Professor, Department of Family & Community Medicine,
University of Toronto
Community-based Family Physician
Past-president, Federation of Medical Women of Canada,
Board member, Immunize Canada
Nora Cutcliffe, MSc, PhD
Medical writer and Consultant, primarily in the field of immunization
Samarpita Das, BSc, 3rd-year medical student
Faculty of Medicine, Vancouver-Fraser Medical Program,
University of British Columbia
Pamela Liao, BSc Hons, MD, CCFP
Assistant Professor, Department of Family and Community Medicine,
University of Toronto
1. Why is TD significant and why should primary care clinicians intervene to minimize patient risk?
Travellers’ diarrhea (TD) is the most common travel-related illness. Although the disease is usually self-limiting, TD can result in many adverse consequences, including inconvenient changes in itinerary, lost time and money, as well as longer-term medical complications.1 Appropriate management of TD during and after a journey remains an important clinical challenge – not only to protect patient health, but also to minimize demand on healthcare resources, both abroad and domestically.2
The goal of this paper is to highlight the significance of TD and review current guidelines for prevention and treatment interventions. The need for education applies to family physicians, nurses, pharmacists and other primary care clinicians who counsel a broad range of travellers, and is not simply an issue for travel-medicine specialists. As the first (or only) point of contact for patients – often just a few days/weeks before travel – primary care practitioners play a pivotal role in providing basic recommendations regarding immunization and medications related to TD. A comprehensive pre-travel consultation also provides an opportunity to discuss other itinerary-specific health risks and appropriate precautions (e.g. surrounding sexually transmitted infection, altitude sickness, etc.) and to ensure routine vaccinations are up-to-date.3 The need to advise travellers on relevant risk management strategies is likely to grow in the near future, since international travel by Canadians is projected to rise 4% per year until 2020, and 27% of surveyed travellers have reported plans to seek medical guidance prior to their trip (e.g. for summer 2017).4
2. How is TD currently defined and what symptoms are associated with acute illness?
Classical TD has been defined as the passage of three or more unformed stools per day, with at least one accompanying symptom including: nausea, vomiting, abdominal cramps or pain, fever, or blood in stools (dysentery).5 In 2017, new definitions for acute TD were put forward by the International Society of Travel Medicine (ISTM) based on functional impact on travel activities, rather than frequency of unformed stools per day, as follows:1
• Mild diarrhea – tolerable, not distressing, and does not interfere with planned activities.
• Moderate diarrhea – distressing or interferes with planned activities.
• Severe diarrhea – incapacitating or completely prevents planned activities; all dysentery.
TD is mainly acquired by ingesting fecally contaminated food or beverages. The most common causative agents are bacterial (80-90%), viral (5-8%), and parasitic (~10%).6 Of the bacterial pathogens, enterotoxigenic Escherichia coli (ETEC) is the most frequent, as detected in 30.4% of TD cases studied worldwide.7,8 Many strains of ETEC produce a heat-labile enterotoxin (LT), similar to cholera toxin, that can mimic the effects of cholera toxin on intestinal mucosa in inducing watery diarrhea.8 This structural similarity explains why the cholera/ETEC-diarrhea vaccine (consisting of killed whole-cell cholera strains plus recombinant cholera B-subunit; WC-rBS) provides modest (50-67%) cross-protection against diarrhea caused by LT-producing ETEC.8,9
The incidence of TD is reported to be 30-70%, depending on destination and season of travel,6 with 12-50% of travellers experiencing incapacitation for part of their trip due to TD.5 In adults, the onset of TD symptoms typically occurs within the first 3-4 days of travel, and the duration of untreated acute TD generally averages another 3-7 days.5,6
3. What about long-term complications, and what other emerging issues may prompt rethinking of TD prevention and treatment?
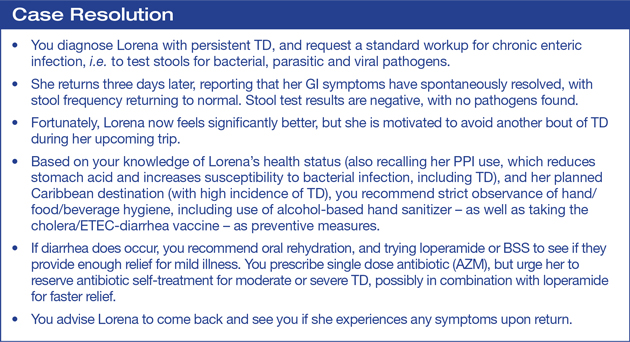
Potential consequences of TD may extend beyond the acute illness, with 2-10% of patients experiencing persistent diarrhea5 – defined as lasting two weeks or longer1 – which may trigger medical visits by returned travellers. Moreover, there has also been increasing recognition of serious long-term complications of TD,2 including post-infectious irritable bowel syndrome (PI-IBS) in 5-10% of TD cases.5 In patients with PI-IBS, symptoms of unpredictable diarrhea, chronic abdominal discomfort, and changes in bowel function may persist for months or even years after the inciting infection.10 As such, patients frequently require follow-up testing and colonoscopy, although evaluation for microbial etiologies and underlying GI disease often remains negative.1 Reactive arthritis (ReA) and Guillain-Barré syndrome (GBS) have also been reported as long-term complications following TD infection.10
Emerging Factors in TD Management
i) Emerging data (summarized above) suggest that clinicians must be aware of both acute and longer-term disabling sequelae of TD, including PI-IBS; these potentially serious consequences beg the need for proactive intervention with prophylactic and therapeutic approaches for management of this disease.
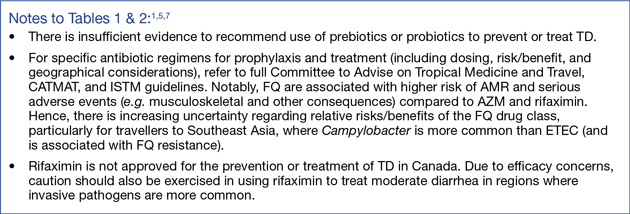
ii) The growing recognition of antimicrobial resistance (AMR), as also associated with antibiotic use in the management of TD1 – and corresponding concerns regarding impact on individual and global population health11 – suggest that use of antibiotics should be recommended with caution and reserved for higher-risk patients.2
iii) The indication for the oral cholera/ETEC-diarrhea vaccine has recently been revised to clarify its use in preventing diarrhea caused specifically by cholera and ETEC.12 Thus, the vaccine is not routinely recommended to prevent all-cause TD;5 it should be viewed as a tool to help reduce (but not eliminate) the risk of ETEC-diarrhea during travel. [Notably, the vaccine is estimated to provide 23-25% overall protection against all-cause TD,9 since < 50% of TD cases are caused by ETEC3,7 and the vaccine provides 50-67% efficacy against TD caused by LT-producing ETEC.8,9 Thus, vaccine efficacy depends on incidence of ETEC at the destination.]
4. What are the current recommendations for appropriate management of TD?
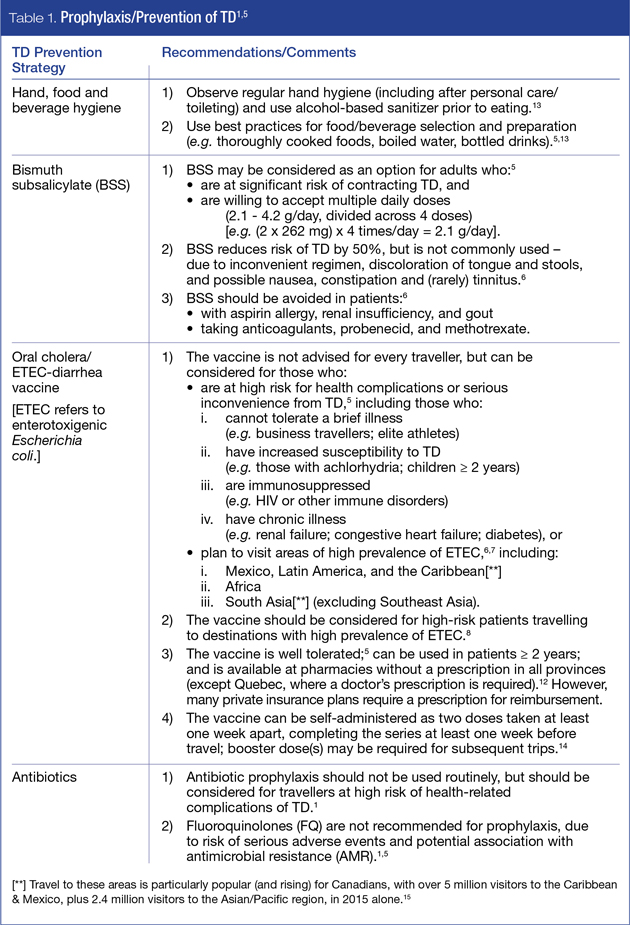
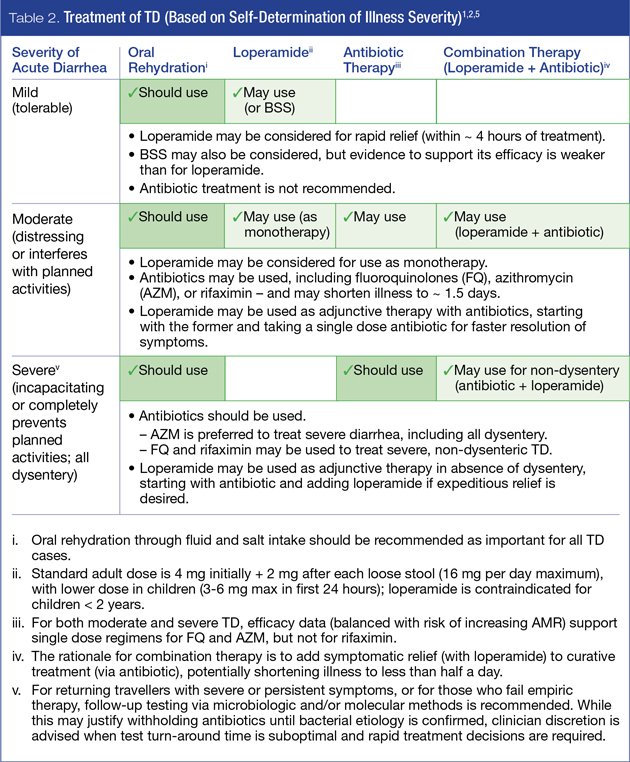
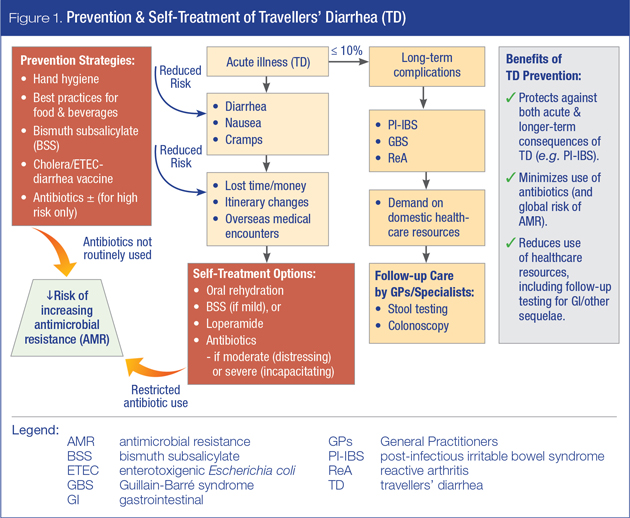
Since TD is caused by a broad spectrum of pathogens, there is no single all-encompassing solution for disease management. However, recent guidelines have been put forward by CATMAT (2015)5 and ISTM (2017)1 to assist with appropriate selection of current prevention and/or treatment options for TD, as summarized in Tables 1 and 2, respectively. An overview of prevention and self-treatment strategies in the broader context of adverse health and other consequences associated with TD is presented in Figure 1.
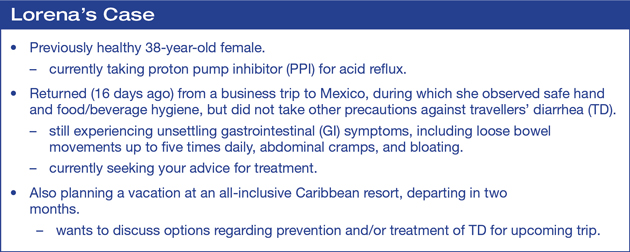
Several factors affect the overall risk of acquiring TD and the severity of symptoms – the most critical of which are patient baseline health status (i.e. age, medical conditions and/or medications) and travel itinerary (i.e. destination, duration, potential exposure to pathogens). These factors should thus be reviewed with travellers in the context of guidelines presented herein. Pre-travel counseling should also include a discussion of the need to balance efficacy and safety of proposed options (including the risk of AMR associated with antibiotic use) as well as patient preferences and ability to comply with recommended self-care regimens.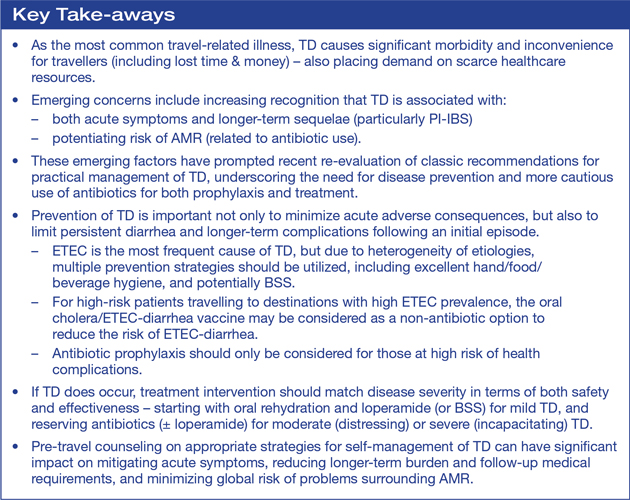
References:
1. Riddle MS, Connor BA, Beeching NJ, et al. Guidelines for the prevention and treatment of travelers’ diarrhea: a graded expert panel report. J Travel Med 2017; 24(suppl_1):S57-S74.
2. Taylor DN, Hamer DH, Shlim DR. Medications for the prevention and treatment of travellers’ diarrhea. J Travel Med 2017; 24(suppl_1):S17-S22.
3. Aw B, Boraston S, Botten D, et al. Travel medicine: what’s involved? when to refer? Can Fam Physician 2014; 60(12):1091-103.
4. Kohane J. Pharmacists help travellers get on their way. PharmacyU 2017; Available at pharmacyu.ca/2017/07/27/pharmacists-help-travellers-get-on-their-way-safely/. Accessed November 2017.
5. Libman M, Bui Y, McDonald P, Steensma C. Committee to Advise on Tropical Medicine and Travel (CATMAT). Statement on Travellers’ Diarrhea. Canada Communicable Disease Report (CCDR) 2015; 41(11):272-85. Available at www.canada.ca/en/public-health/services/travel-health/about-catmat/statement-travellers-diarrhea.html. Accessed November 2017.
6. Centers for Disease Control and Prevention (CDC) Yellow Book 2018: Health Information for International Travel. New York: Oxford University Press 2017. Chapter 2, Traveler’s Diarrhea.
7. Shah N, DuPont HL, Ramsey DJ. Global etiology of travelers’ diarrhea: systematic review from 1973 to the present. Am J Trop Med Hyg 2009; 80(4):609-14.
8. Jelinek T, Kollaritsch H. Vaccination with Dukoral against travelers’ diarrhea (ETEC) and cholera. Expert rev vaccines 2008; 7(5):561-67.
9. Public Health Agency of Canada, Committee to Advise on Tropical Medicine and Travel (CATMAT) and National Advisory Committee on Immunization (NACI). Statement on New Oral Cholera and Travellers’ Diarrhea Vaccination, Canada Communicable Disease Report (CCDR) 2005; 31:1-12.
10. Connor BA, Riddle MS. Post-infectious sequelae of travelers’ diarrhea. J Travel Med 2013; 20(5):303-12.
11. Government of Canada, Tackling Antimicrobial Resistance and Antimicrobial Use: A Pan-Canadian Framework for Action. 2017; Available at www.canada.ca/en/health-canada/services/publications/drugs-health-products/tackling-antimicrobial-resistance-use-pan-canadian-framework-action.html. Accessed November 2017.
12. Valneva Canada Inc. Updated indication for Dukoral® travel vaccine: as Canadians take a budget-conscious approach to tropical destinations in 2016, Enterotoxigenic E. coli is a growing health risk. Press release, May 9, 2017. Available at https://www.valneva.ca/media/Press_releases/News_release__Dukoral_April_29_FINAL_Layout_EN.pdf. Accessed November 2017.
13. Huston P. Treatment and prevention of traveler’s diarrhea. Can Fam Physician 2015; 61(11):976.
14. Valneva Canada Inc. Dukoral® product monograph. Date of Approval: December 22, 2015.
15. Tourism Intelligence Network. Overview of Canadian Outbound Travel, Dec. 7, 2016; Available at http://tourismintelligence.ca/2016/12/07/overview-of-canadian-outbound-travel/. Accessed November 2017.
Development of this article was made possible through the financial support of Valneva Canada Inc. The opinions expressed herein are those of the authors, and do not necessarily reflect the views and opinions of Valneva Canada Inc. The authors had complete editorial independence in the development of this article and are responsible for its accuracy. The sponsor exerted no influence in the selection of content or material published.